|
November 2008 |
Volume 2, Issue 5 |
|
What is Your Target Postural Zone?
|
If you go to a physical therapist or chiropractor for nearly any musculoskeletal problem, a core part of their routine examination will include an assessment of standing and sitting posture. Their training has mandated this assessment because their professions consider postural abnormalities and loads to be a significant factor in musculoskeletal health. For them, to overlook posture is to miss the forest for the trees. They know that posture correction is essential to restoring function and that posture is in a constant battle against gravity. This is not an arbitrary focus or fanciful notion: everybody, especially the mechanical engineer, understands the powerful effects of gravity over time. Gravity causes even the grandest of human architectural designs to crumble eventually to the ground.
Given all the theory and research written about foot biomechanics, one might expect to find more emphasis on the importance of foot posture with respect to function. To date, there is a dearth of knowledge regarding the posture of the foot as it relates to dynamic function. The average person on the street can notice if someone has flat feet. The practicing podiatrist notes the collapse of foot architecture all day long. Yet nowhere in our most learned discussions is the collapsed arch of the foot seen as a primary concern when discussing functional intervention with an orthotic. This is in spite of the accepted fact that feet should re-supinate after midstance. Can there be any re-supination without a change in posture? In fact, some of the most pre-eminent lecturers in podiatric biomechanics focus only on “tissue stress reduction” by any means other than restoring a functional posture to the foot. Apparently, the conventional wisdom believes that it is either not possible or not necessary. However, we abandon this elemental precept of musculoskeletal health at our professional peril. To help understand the importance of foot posture, I present the following postural zone categories that link our intervention strategies to expected postural results and clinical outcomes. (Note: these zones define qualitatively different, as opposed to absolute, levels of postural correction that will vary quite a bit from foot to foot.)
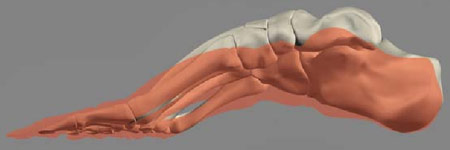 |
Relative arch heights of Neutral Position (red) vs. MASS Position.
|
This is the most common target zone utilized for flexible, over-pronating feet. Low orthotic arches allow the foot to pronate into the end ranges of available pronation. Posts, skives, inverted casts, etc. try to dampen the last one degree or so of pronation to avoid excessive tissue stresses. Plantar foot soft tissues and ligaments also assist in dampening pronation. At this level of support and dampening, symptoms may be relieved but function is not improved, especially in terms of re-supination after heel lift. There will be no observed changes in foot posture standing on and off a device modeled for pathological zone control. The foot is allowed to pronate even lower than neutral position since cast correction is the norm rather than the exception in most Rootian labs. Symptoms may be alleviated temporarily, but, since the biomechanical disease continues unabated, are likely to return along with advancing deformity. Dispensing a pathological zone level of care is equivalent to getting a temporary filling at the dentist or a partial cardiac bypass.
If we were to follow neutral position methodology to the letter, we might correct foot posture up to the dysfunctional zone. By most current standards, this would require what would be perceived to be a high-arched orthotic (without cast correction). However, since the foot was cast only to neutral supination, there will still be a good distance for the foot to fall into pronation before slamming into this now relatively high arch. The good news is that more pronation is arrested; the bad news is that the patient now complains of discomfort from slamming into this more prominent arch. It is exactly this scenario that probably led to the practice of arch fill and the avoidance of high-arch orthotics in the first place. Sadly, there is still not enough correction at this postural level to insure adequate re-supination after heel strike. The physics of bringing the arch back up to full, functional supination is still too daunting for the average flexible, over-pronater. Even so, the dysfunctional zone defines the upper limit of where conventional orthotics dare to go. It seems we have been arbitrarily limited and distracted by the artificial barrier of neutral position for a long time. And, ironically, it has been forcing us back into the apparent comfort of the pathological zone and the interchangeable value of a custom or a prefab.
 |
Side by side comparison of relative arch heights in the Pathological (red), Dysfunctional (yellow), Functional (green) and Supination Instability (violet) zones.
|
OK, so how high do we have to go? Would it not be dangerous to guess at some arbitrary arch height just for the sake of re-supination? Yes. That is why the MASS Position casting standard is so useful: let the foot tell us how high it should go. If we use the floor as a frame of reference, supinate the foot as much as possible while maintaining floor-level contact with the heel and forefoot, any individual foot will tell us how high the arch should be and the custom shape of the person’s plantar vault. This is the functional posture zone. If we support the foot in this position with enough rigidity for posture control but enough flex to yield somewhat on impact, the foot easily has enough supination, as a starting point in late midstance, to achieve functional re-supination after heel lift. This is because the talar head, in MASS position, is resting near a level anterior facet. Very little effort is then needed to move the head into its locked position on top of the anterior facet. The functional zone is that postural range in which the subtalar joint has minimal supination resistance.
It is possible to over-supinate and over-correct a foot. When there is so much tarsal supination that the forefoot inverts relative to the floor, the foot is too supinated. There will be a tendency for increased inversion moments at the ankle at heel strike that can cause lateral ankle sprains. There may also be some difficulty in getting sufficient load on the first metatarsal head. So, while there is a need for significant supination correction with most feet, it is possible to overdo it and cause a new set of problems. This is another reason why guessing corrective arch height is a bad idea.
Again, the idea that correct posture is essential to normal function is a universally acknowledged truth in all musculoskeletal professions. If podiatry wants to claim the highest level of expertise on foot function, it will have to re-examine the dysfunctional assumptions that now govern the prescription and manufacture of corrective foot orthoses. MASS position theory is a credible first step in that direction because it supplies a methodology for determining the optimally corrected posture for any individual foot.
|